Panoramic Sysnthesis of the Onchocerciasis Control Program in West Africa – Roma, 18.11.1992
Gambia
Ebrahim M. Samba
Premio Balzan 1992 per la medicina preventiva
Per il suo ruolo di guida nella lotta contro l’oncocercosi (cecità dei fiumi) nell’Africa Occidentale. In seno all’Organizzazione Mondiale della Sanità ha diretto il Programma di Controllo per l’Oncocercosi, grazie al quale si sono potuti proteggere dalla malattia centinaia di migliaia di esseri umani, prevenendo il pericolo della cecità. Il successo del programma ha permesso la ripopolazione di larghe e fertili regioni e ha perciò avuto importanti conseguenze sociali ed economiche per i paesi partecipanti.
Ebrahim M. Samba:
Foreword
The Onchocerciasis Control Program in West Africa – OCP in common parlance – is in many ways unique. Public health activities are implicitly understood to promote socioeconomic development, an understanding which is rarely spelled out in explicit terms. However, in the case of OCP, the importance of controlling river blindness for the sake of removing a serious obstacle to agricultural production is at par with the intent to rid the afflicted populations of an age-old scourge. The Program objective thus calls for the elimination within the OCP area of onchocerciasis as a disease of public health importance and “as an obstacle to socioeconomic development”.
Also, the timeframe of the Program is exceptional. Given that an extended period of control is required to bring the human reservoir of the parasite to an insignificant level, it was understood by all parties, Participating Countries and Donors alike, that operations would continue uninterruptedly for 20 years. This time perspective has rarely, if ever, been matched by other operational pro grammes conducted within the framework of the United Nations system.
The Onchocerciasis Control Program is one of the largest inter-country undertakings implemented by the World Health Organization. The Program spans over eleven countries with a highly mobile staff attached to operational centers strategically located wherever control activities are going on. Aerial operations are conducted along a:river network which totals 50, 000 km and OCP staff throughout the Program area carries out continuing entomological surveillance, monitoring of river flows and of the aquatic environment, epidemiological valuation and community-wide distribution of ivermectin tablets 6 mg (Mectizan R, Merck).
ONCHOCERCIASIS AND ITS IMPACT
Initially onchocerciasis was discovered and described by Leuckart (a German medical missionary) who observed the disease in Cote d’Ivoire in 1893.
Sir Albert Cook reported the occurrence of onchocerciasis in Uganda in 1899 and Robles discovered the disease in Guatemala in 1915 while Pacheco Luna reported its association with blindness in 1919. Onchocerciasis was first detected in Northern Nigeria by Budden in 1952.
The agent and clinical manifestations of onchocerciasis
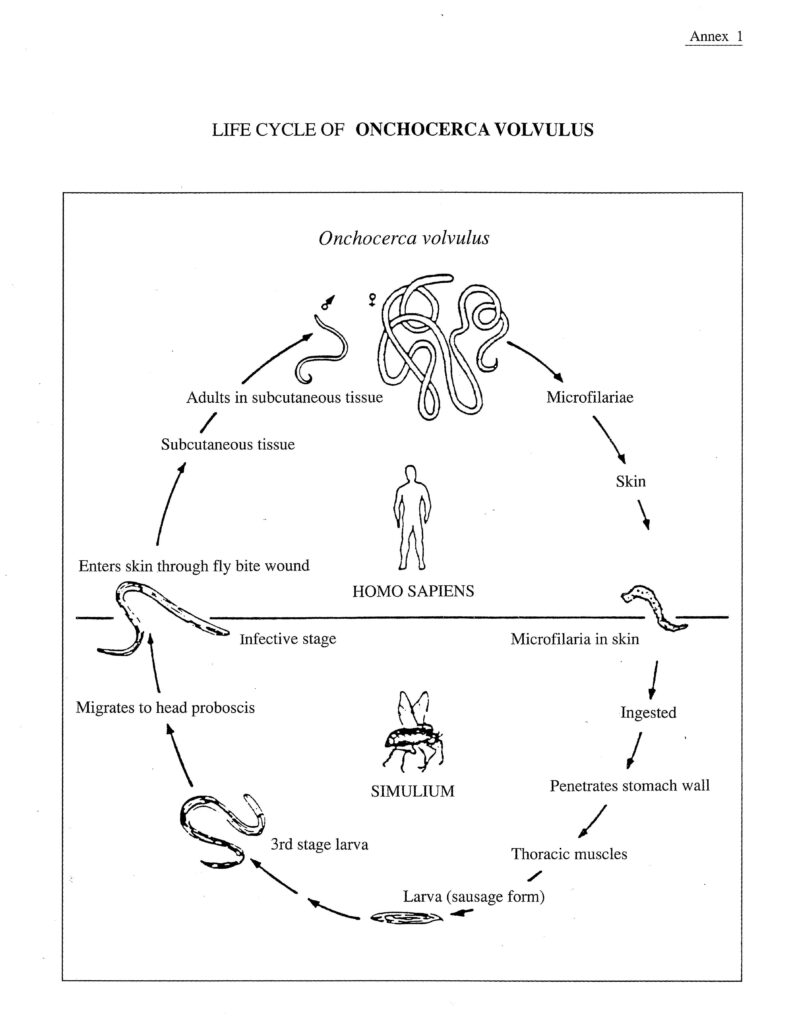
Onchocerciasis is a parasitic disease caused by a filarial (threadlike) worm, Onchocerca volvulus, of which the adult females (macrofilariae, 40-45 m long) lodge in nodules under the human skin although they can be found free in subcutis. In Africa the nodules are commonly distributed around the pelvis particularly over the iliac crest, femoral trochanter, coccy, sacrum and the lateral chest wall.
When fertilized by the smaller male, the females can during an average lifetime of 12 years produce millions of microscopic embryos (microfilariae, about 0.3 mm length) which live around two years and give rise to the clinical mamfestations of the disease.
The microfilariae are found in the intercellular fluid, including that of the ye, and their death and subsequent disintegration result in inflammatory reactions which in the eye may lead to serious visual impairment, including blindness, in the microfilarial load is high following a prolonged period of exposure to massive infection. Mortality among the blind may be four times as high as for nonblind of the same age and in the same community.
In addition, the microfilariae give rise to intensely itching rashes, to wrinkling, thickening and depigmentation of the skin, to lymphadenitis resulting in hanging groins and elephantiasis of the genitals, and to generai debilitation, including loss of weight.
The vector and its transmission of the agent
The microfilariae are transmitted from one person to another by blackflies belonging in Africa to the Simulium damnosum species complex. The female lays its eggs (several hundreds per batch) at, or below, water surface in fast-flowing rivers where they hatch after 36 to 48 hours. The larval stage which lasts 5 to 10 days (depending on the water temperature) is followed by pupation and the emergence of adults after further 2 or 3 days. The blackfly lives up to four weeks and can cover several hundred kilometers in flight.
The female blackfly mates only once, namely on the day following emergence. She then seeks a bloodmeal, which is necessary for the maturation of her eggs, and is ready for oviposition 4or 5 days after the meal. If this is taken from a person infected with onchocerciasis, microfilariae may be ingested with the blood. They do not multiply in the blackfly and only one or two of them develop during 6 to 8 days from asexual microfilariae into infective larvae (L3) capable of becoming sexually mature adults in the human host. This development is completed only by the time of the third bloodmeal and, consequently, for the blackfly to function as a vector it must survive the laying of two batches of eggs.
Once infective larvae (L3) are injected into a human host during a blood meal, they might develop into adults producing microfilariae which may in tum be ingested by blackflies thus completing the life cycle of the parasite (see Annex 1). The time between the entry of larvae (L3) and the appearance of onchocercal symptoms, the incubation period, varies from one to three years.
Control of transmission and of onchocercal manifestations
Larviciding of the breeding sites of the blackfly larvae is, presently, the only means of interrupting transmission to the extent that the human reservoir of Onchocerca volvulus will eventually die out and will remain so until such time as elimination of the adult worm can be achieved by community-wide application of chemotherapeutic agents.
Until recently, only two anti-onchocerciasis compounds have been used for treatment purposes. Diethylcarbamazine (DEC), developed in 1943, is a microfilaricide (kills microfilariae) and must therefore be given repeatedly as long as the patient harbors fertile female worms. It provokes severe and sometimes dangerous systemic (Mazzotti) reactions and can aggravate existing, or precipitate new, ocular lesions, all as a result of the sudden, massive death of the microfilariae.
Suramin, available as from 1920, is a microfilaricide (kills the adult worm) which must be given once weekly for up to two months. It is of restricted use insofar as it can give rise to serious adverse reactions such as anaphylactic shock and kidney, liver and gastro-intestinal complications. Neither DEC nor suramin can therefore be given on a scale sufficiently large to significantly reduce the parasite reservoir in the populations concerned. Their use is limited to the treatment of individual cases under strict medical supervision.
Since 1987 ivermectin tablets 6 mg (MectizanR Merck) with microfilaricidal effect have become available for large-scale distribution in human populations. It has proved itself to be a valuable therapeutic agent, it reduces considerably the risk of blindness, and is easily dispensed under field conditions. Ivermectin does not, however, have the originally hoped for, decisive impact on transmission.
The impact of onchocerciasis on health and socioeconomic conditions
Wherever onchocerciasis establishes itself at a high intensity and strong endemicity level, as has been the case in the savanna belt of West Africa, the disease has been a serious threat to the health of the populations concerned and constituted an impediment to socioeconomic development.
Insofar as the vector is constrained in its flight movements to a relative proximity to rivers presenting potential breeding sites for its larvae, the populations exposed to onchocercal infections are those living alongside the rivers. The colloquial name of the disease “river blindness”, is therefore particularly apt.
In such riverain communities subjected to a high intensity of onchocercal transmission and infection, 60-70% or more of the population could harbor the parasite as demonstrated by the presence of microfilariae in skin snips examined microscopically. At that level of prevalence, up to 10% of the population may be blind as a result of the disease and, perhaps, double or triple of that number could suffer from severe visual handicap. Ocular onchocerciasis is also referred to as Robles disease. When the Onchocerciasis Control Program started in the original seven-country area in West Africa with a total population exceeding 10 million, more than one million was infected by onchocerciasis and 100,000 suffered from its serious ocular manifestations, including a large proportion blinded by the disease.
Given this scale of serious ocular manifestations including blindness, onchocerciasis is obviously an important health problem. But the nefarious effect of the disease extends beyond the sphere of health into the field of economics.
As the exposed populations seek relief from onchocercal infection and disease, they move away from the fertile riverain zones where the risk is highest to the less fertile, upland country, resulting in over-cropping and soil erosion. Also, the threat of blinding onchocerciasis, which is especially serious to adult males, induce young men to migrate to urban areas, thus impairing the productivity and disrupting family life from which infected persons showing skin and other onchocercal manifestations are often excluded due to difficulties in finding marriage partners.
EARLY ATTEMPTS AT COMMUNITY-WIDE CONTROL OF ONCHOCERCIASIS WITH PARTICULAR REFERENCE TO WEST AFRICA
Although the blackfly, Simulium damnosum s.l., was identified as the vector of onchocercal infection in 1926, it was not before the early 1950s that comprehensive entomological and epidemiological studies were undertaken with a view to investigating the possibility of using vector control to interrupt transmission on a scale sufficiently large to have a significant epidemiologic impact.
The conclusion of these field studies and pilot projects was that ground control was quite successful in reducing the biting blackfly population as long as control activities were maintained but the impact on transmission was limited due to the regular influx of the fly from surrounding untreated areas. In other words much larger areas would need to be treated if a lasting effect were to be obtained.
The serious health and socioeconomic repercussions, of onchocerciasis and the emerging indications that control was within reach, encouraged health authorities in the countries most afflicted to invite the scientific community to study the feasibility and operational aspects of a large-scale control program. This led to a major conference held in Tunis, Tunisia, in July 1968 which concluded that large-scale control should be attempted and that such control could be obtained through larviciding, essentially by means of aerial spraying. The conference also emphasized that larviciding would need to be applied continuously fora period of 10-15 years to permit virtual elimination of Onchocerca volvulus from the human population and made specific recommendations for a program suggesting West Africa for its implementation.
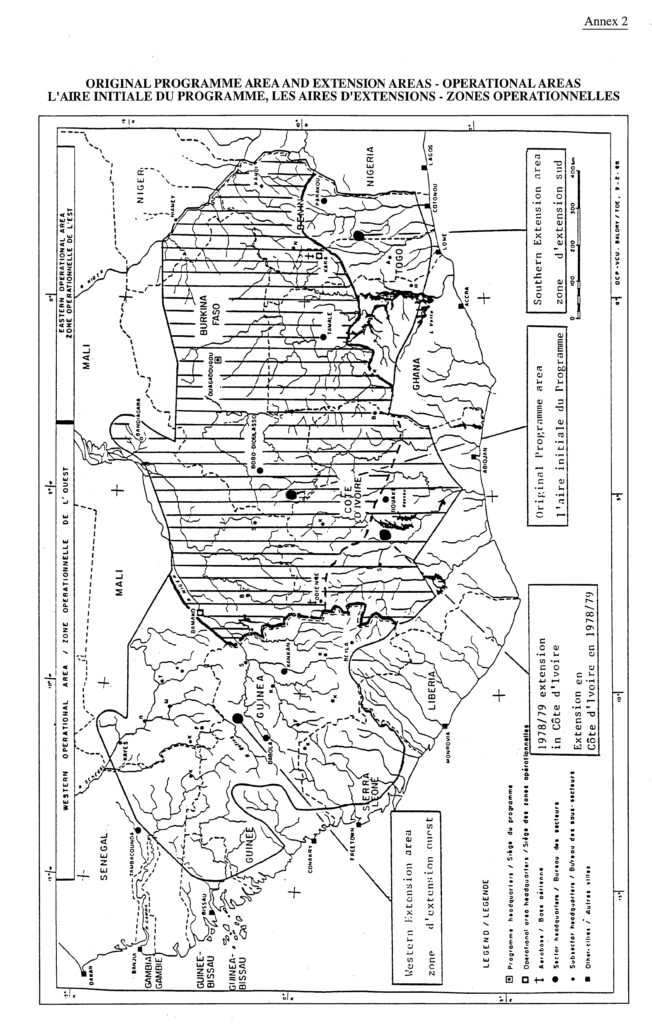
A “study mission”, known as the Preparatory Assistance Mission to the Governments of Dahomey (now Benin), Ghana, Côte d’Ivoire, Mali, Niger, Togo and Upper Volta (now Burkina Faso): the PAG Mission, prepared a plan of work for onchocerciasis control in the area centered on aerial larviciding to interrupt transmission over an area then believed to be sufficiently large to avoid reinvasion of infective blackflies (1) and to be conducted continuously over a period of 20 years (2), at that time considered necessary for the human reservoir of the adult worm to die out in the absence of renewed infection (map of current area of OCP operations in Annex 2).
In the final chapter of the PAG report a blueprint for the structure and management of the Onchocerciasis Control Program was presented with specification of the composition and tasks of various committees and panels, and with a proposed management and organizational chart of OCP. These structures were put in place from the start of operations in 1974.
(I) Their flight range was then estimated at 100 to 150 km only. Later, OCP experience demonstrated that blackflies can cover severa! hundred kilometers in flight.
(2) Fifteen years of OCP-conducted vector contro! has proved that 14 years of uninterrupted larviciding suffices to virtually eliminate the human reservoir of the parasite.
STRUCTURE, FUNCTIONAL ORGANIZATION AND OPERATIONS OF THE ONCHOCERCIASIS CONTROL PROGRAMME
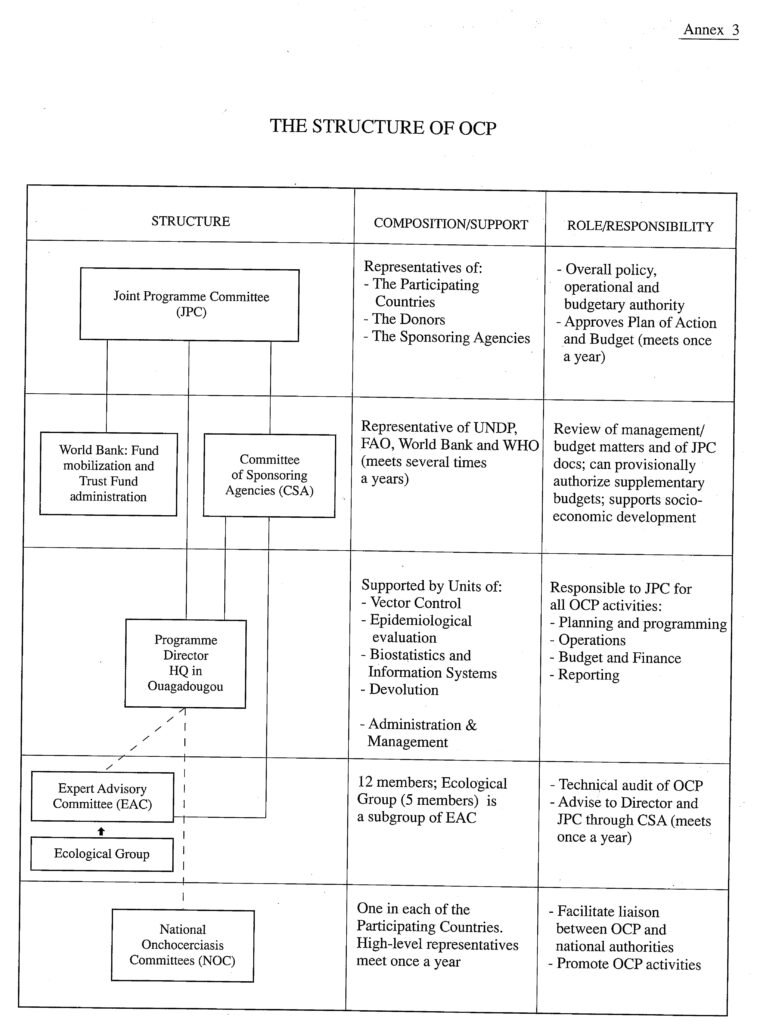
The Onchocerciasis Control Program has developed into a four-tier structure. The uppermost level is that of “directives”, personified in the Joint Program Committee (JPC), which exercises full directional powers as regards overall Program policy, strategy development and budget matters. Next comes the “advisory level” represented by the Expert Advisory Committee (EAC). The third level is that of “support and collaboration” consisting of the Committee of Sponsoring Agencies (CSA); the procurement and administration of financial resources; and the administrative support provided by WHO HQ and WHO/ AFRO. This level also includes collaboration with the Participating Countries. Finally, “operations” concerns OCP sensu strictu as the organ responsible for planning, programming and implementing field operations in conformity with the directives and recommendations emanating from the preceding levels. The four-tier structure is illustrated in the following table (see also Annex 3):
| LEVEL | FUNCTIONS | COMPONENT OF OCP/WHO STRUCTUREINVOLVED |
| l. | Determination of Program policy, agreement on overall directives concerning Program implementation and decision on budget levels. | JPC |
| 2. | Recommendations on scientific, technical and operational matters. | EAC |
| 3. | Support and collaboration monitoring, scrutiny of documents and preparation for JPC sessions, support to management of OCP budget and support to socioeconomic development fund mobilization and Trust Fund administrationadministrative supportcollaboration with Donorscollaboration with Participating Countries | CSA World Bank WHO/HQ, WHO/AFRO Donors’ Meetings National Onchocerciasis Committees (NOCs) |
| 4. | Planning, programming, implementation of, and reporting on, field operations developed on the basis of EAC recommendations and approved by JPC. Responsibility also for budget preparation. | OCP sensu strictu |
Joint Program Committee
The membership of the Joint Program Committee (JPC) includes representatives of the Participating Governments, of the Donors and of the Sponsoring Agencies. Ex officio participants are representatives of the Expert Advisory Committee, of the Ecological Group, and of the WHO External Audit Office. Sessions of the Joint Program Committee, apart from providing the OCP management with guidance in the conduct of, and directives for, Program operations as well as securing the necessary funds, are occasions propitious for dialogues between all the interested parties. Through personal contact with delegates, OCP staff, and in particular the Program Director, keep abreast with the evolving attitude towards OCP of the Participating Countries and the Donor community, their confidence and their worries, all important in the development of program proposals to be considered in the open forum of Committee deliberations.
Expert Advisory Committee and Ecological Group
The Expert Advisory Committee (EAC) with up to twelve members reviews the latest knowledge and scientific information in all fields related to the Onchocerciasis Control Program and makes it available to WHO; analyzes and comments on the technical and scientific reports of the Program and plans of action; and makes recommendations designed to improve the planning of the Program and the implementation of its activities. The task of the Ecological Group (five members) is to study “the ecological impact on the environment of the use of insecticides in the Program”.
The importance for the Program of independent advice is indisputable. Not only do the EAC and Ecological Group provide the Program management with scientifically and technically viable advice as to the conduct of OCP operations, but the Joint Program Committee is constantly reassured by outside experts that the Program is on the right course and that the methodology applied is sound, environmentally safe and cost/efficient.
The Committee of Sponsoring Agencies
The Committee of Sponsoring Agencies (CSA), with members from UNDP, FAO, World Bank and WHO, is an organ of preparation and execution. It reviews the work plans and budgets prepared by the Executing Agency (WHO), is responsible for preparing the Onchocerciasis Fund Agreements and is associated with long-term planning, medium-term programming and review/evaluation exercises.
This Committee has over time proved its value as a monitoring and steering group, fully living up to what has been expected of it, namely to identify and present operational and administrative issues facing OCP; to assess the capacity of the Program to resolve such issues; and to make recommendations to effectively assist JPC in decision-making.
The Onchocerciasis Fund
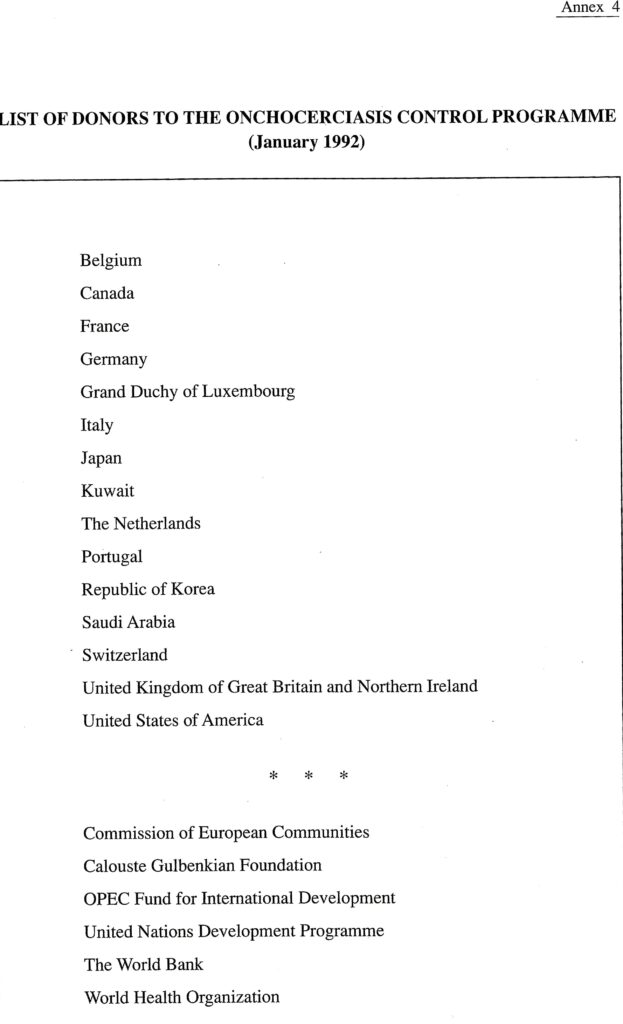
The 1979, 1986 and 1992 Onchocerciasis Fund Agreements, each covering a six-year period (second, third and fourth Phases of the Program), set forth the amounts pledged by individual Donors for the entire period or, in some instances, for the first year with an indication of the likely contributions for the following years. An up-to-date list of Donors to the Program is attached as Annex 4.
The efforts of the World Bank to raise the funds required to keep OCP on its set course are of critical importance for the Program. The Bank has appointed one of its officers to handle OCP matters on a full-time basis. One of his main tasks is to maintain continuing contact with existing and potential Donors with a view to soliciting contributions. This is particularly important during the period, once every six years, when a new Fund Agreement is being prepared and when the Contributing Parties need to be sounded out as to their reaction to the activities planned for the next Financial Phase and to their budgetary implications.
Collaboration with the Participating Countries and with the Donors
The Onchocerciasis Control Program has, since its beginning, been seen by the Participating Governments, their populations and the Donors, as a program tackling a health and socioeconomic problem ranking high on the list of priorities. Furthermore, the achievements of the Program in terms of interruption of transmission and a drastically Jowered onchocercal morbidity have been such as to ensure whole-hearted collaboration, not only with the national authorities and Dono s but also, most importantly, with the people at the village level.
The collaboration between the Program and the Participating Countries has been altogether satisfactory. The Governments have amply fulfilled their obligations and in several instances gone beyond their contractual commitments. Part of OCP’s collaboration with Participating Countries is channelled through National Onchocerciasis Committees (NOCs), active, at varying degrees and in different disciplines, in supporting the Program and its activities at the national level.
There are several opportunities for discussions with the Donors concerning funding of the Program e.g. during sessions of the Joint Program Committee, during Doriors’ Conferences called and òrganized by the World Bank whenever required, in particular in connection with the preparation of a new Onchocerciasis Fund Agreement, and on the occasion of meetings with individual representatives of the Donor Community. The most effective approach, however, is that of visits by the World Bank official concerned with OCP, accompanied by the Program Director, to the capitals of Donor countries and to headquarters of contributing organizations and agencies.
Collaboration with institutions and bodies external to the Program structure
Given the importance of larviciding in the OCP control strategy, the Program maintains close contact with the chemical industry with a view to encouraging the identification and development of new larvicides and improvement of existing ones. It is due to this collaboration that the Program has been able to overcome the problem of lowered susceptibility to organophosphorus compounds by employing replacement larvicides in rotation and to ensure the absence of ecological damage by aerial spraying. Another example of a close working relationship with industry is the search for chemotherapeutic agents where the OCP/TDR (1) funded Onchocerciasis Chemotherapy Project (OCT/ Macrofil) plays a coordinating, supporting role relying on pharmaceutical firms to carry through the testing and screening process up to the clinical stage for which OCT assumes responsibility.
An especially close relationship has been established during the last few years with some Non-Governmental Organizations (NGOs) and Private Voluntary Organizations (PVOs) particularly active in the field of prevention of diminished eye-sight and blindness. The collaboration with NGOs and PVOs centers on large-scale application of ivermectin could eventually extend to the support of national efforts in the field of devolution.
(I) Special Program of Research and Training in Tropical Diseases (WHO/UNDP/World Bank)
Involvement of well-known personalities
A visit in 1972 by the then President of the World Bank, Mr. Robert McNamara, to West Africa made him realize the glaring need for controlling river-blindness, not only on humanitarian grounds but also as an investment in socioeconomic development. His conviction of the necessity of bringing about an inter-country effort to control the disease became a driving force in the preparations for, and launching of, the Program.
Another good illustration of the active involvement of internationally known personalities in OCP operations was the appointment of Dr. M.G. Candau, a former Director-General of WHO, as the Independent Chairman of the Joint Co ordinating Committee (the forerunner of the Joint Program Committee) from 1975 to 1980. Dr. Candau, with his twenty years as Executive Head of one of the largest and most successful Specialized Agencies within the United Nations system, brought with him to OCP a highly developed political flair, a vast experience in the field of management and a good understanding and pragmatic approach to technical and operational issues.
Other examples are the chairmanship of the Economic Development Advisory Panel (disestablished in 1979) in the person of Paul-Marc Henry, Director of the OECD Development Centre, who had held top posts in the UNDP secretariat and that of Guy Camus, at that time Director-General of ORSTOM (1), who became a member of EAC from 1980-1982 and its chairman in 1980 and 1981. Also, the membership of other OCP committees has been inclusive of many scientists and experts of worldwide renown.
(1) French Institute of Scientific Research for Development through Cooperation.
OCP functional entities and their operations
Office of the Program Director
The Program Director organizes, c ordinates and supervises all OCP activities, ensures continuing contact with the Donors and the Participating Countries, arranges for documents to be considered at the various OCP meetings and, since the early eighties, supports the preparation for, and implementation of, the devolution process, an activity of ever increasing importance, lately in the hands of a newly created Devolution Unit.
Vector Control
The Vector Control Unit (VCU) has four main functions: to carry out entomological surveillance with a view to guiding aerial operations according to the observed presence or absence of infective blackflies; to conduct aerial larviciding for the purpose of interrupting transmission of infection; to achieve virtual elimination of the human reservoir of the parasite; to monitor the environmental effect, if any, of OCP operations and, if required, to adjust such operations to avoid damage to the non-target fauna; and to conduct research on the disease vector conducive to enhanced effectiveness of its control as well as on insecticide compounds and their formulations with a view to improving the Program’s capability to deal with lowered susceptibility to insecticides.
Entomological surveillance is based on a Program-wide system of sectors and sub-sectors, the latter being grouped around, and supervised by staff of the former. The sectors (7) and sub-sectors (31) are responsible, at different levels of competence, for checking the absence or determining the presence of blackfly larvae in rivers under treatment (effect of larviciding); for capturing blackflies for identification and dissection to ascertain their infectivity according to the presence or absence of Onchocerca volvulus in larval stages; for reading water gauges to decide on the frequency and periodicity (usually weekly) of larviciding; and for evaluating its impact – all in order to provide the data necessary for conducting aerial operations.
The aircraft fleet, originally stationed at Bobo-Dioulasso airport and Tamale, Ghana, but since 1983 based in Kara, Togo, and in Odienné, Cote d’Ivoire, consists of up to eleven helicopters, the actual number depending on the season, and two fixed-wing and one liaison aircraft. The fleet, its pilots and mechanics are provided under a three-year commercial contract with an aerial spraying company after call for tenders. Aerial operations are centrally coordinated from OCP headquarters in Ouagadougou, Burkina Faso, by means of the radio-telephone system connecting the entomological surveillance network with the Vector Control Unit (VCU). The possibility of widespread aerial application of insecticides producing an adverse effect on the environment, in particular on non-target organisms, has been of continuing concern to the Program.
The total area under vector control in the Original Program area covered 654, 000 km2 to which would be added 110, 000 km2 in the soutern part of Cote d’Ivoire where larviciding started 1978/1979. By that time 18,000 km of river was under vector control protecting a population of 16.5 million. The phased expansion of vector control into the Southern and Western Extension areas brought the total OCP area to 1,235,000 km2 with a population of 30 million and increasing the length of rivers under control to 50,000 km.
Epidemiological evaluation
Until 1988, the activities of the Epidemiological Evaluation Unit (EPI) were essentially oriented to an assessment of the impact of vector control, by means of repeated examination of indicator villages consisting of the search for microfilariae in skin snips, visual testing, and ophthalmological examination. The data obtained from these evaluations allow for the computation of the prevalence, community load of infection and incidence, all indices which have taken on added importance in the determination of where and when onchocerciasis has reached the level below -which larviciding can cease. With time, the EPI unit has added to its original tasks such activities as the study of the longevity of the adult Onchocerca volvulus; investigation of forest onchocerciasis; the search for field applicable immunodiagnostic tests and DNA differentiation of parasite strains; field testing of ivermectin and its application on a community-wide scale; and, more recently, participation in decision-making regarding cessation of larviciding and support to epidemiological surveillance in respect to the detection and control of recrudescence.
Statistics and information support
The unit of Biostatistics and Information Support (BIS) has developed a predictive epidemiological computerized model which has been of critical importance for preparing OCP’s long-term and medium-term plans. One of the main conclusions of model simulations was that 14 years of larviciding is required to virtually eliminate the human reservoir of the adult onchocercal worm, a prediction on which the timeframe for future operations is based. Furthermore, simulations have shown that effective ivermectin distribution can cope with recrudescence, provided such distribution is instituted soon after the appearance of recrudescent infection. Other uses of the epidemiological model are its role in determining the epidemiological level at which larviciding can cease and the predictions of onchocercal manifestations in the eye in order, inter alia, to anticipate the long-term effect of ivermectin treatment.
On the information-support side, OCP/BIS has been instrumental in setting up a Program-wide computer and wordprocessing network as well as undertaking the training of the staff concerned at OCP headquarters and in the Program’s operational centers.
Devolution and training
Conceptually, devolution should be seen as national maintenance (after cessation of Program operations) of OCP achievements through active epidemiological surveillance aiming at early detection of foci of recrudescent infection/disease, and the control of such recrudescence by ivermectin treatment. The role of OCP in the field of devolution is one of training, support and coordination. More specifically, the Program assists in the drawing up of devolution plans; provides technical guidance as regards epidemiological surveillance and recrudescence control; trains nationals in multi-disease surveillance, drug distribution and management; and conducts operational research on devolution-connected activities including the long-term impact of ivermectin distribution. To cope with these tasks, OCP established in 1991 a Devolution Unit as its headquarters in Ouagadougou. Furthermore, the Director of the WHO Regional Office for Africa has appointed an intercountry Coordinator for devolution, stationed in the WHO Representative’s office in Ouagadougou, and set up a devolution Task Force including AFRO and OCP staff, the Coordinator and OCCGE (1).
While OCP training, was, by necessity, initially oriented towards preparing national and OCP staff to work in onchocerciasis control as such, the emphasis has recently shifted to training nationals in the key disciplines of devolution. The trend over the years has thus been a move from awarding fellowships in subjects relating to vector control to giving training grants in such fields as epidemiology, biostatistics, management and public health administration. With time, the selection of teaching institutions has increasingly centered on those located in Africa so that today, practically all fellowships granted by the Program are directed to African teaching centers at a cost four to five times lo wer than that of sending fellows to Europe or North America.
(1) Organisation de Coordination et de Coopération pour la lutte contre les Grandes Endémies
Research
The OCP-conducted/supported research and field investigations are concerned with problem-solving managerial issues in practically all fields of operations with particular emphasis on vector control and epidemiology. To this should be added devolution which has recently become a subject for intensive operational research. When it comes to the longer-term and more theoretical, basic research of potential importance to the Program, OCP maintains close contact with the WHO/U DP/World Bank Special Program of Research and Training in Tropical Diseases (TOR), with other interested programmes at WHO head quarters, with universities and with industry.
OCP established in 1982 the Onchocerciasis Chemotherapy Project (OCT) to develop “an effective, low-cost and safe drug for treatment of onchocerciasis which would permanently sterilize or kill adult female Onchocerca volvulus“. The project has recruited participation of chemical and pharmaceutical companies in drug development, solicited candidate compounds from academia and other scientific institutions and funded research contracts to synthesize compounds based on biochemical rationals or lead-directed synthesis.
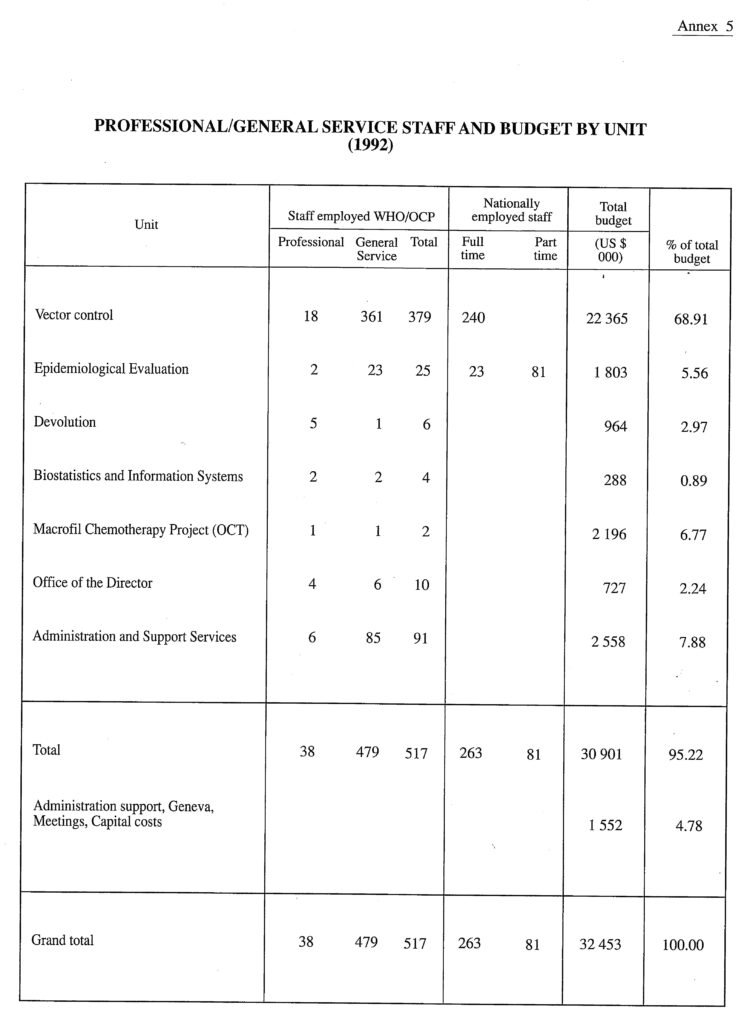
Administration and support services
The unrelenting efforts of the OCP management and administration to implement operations at the lowest possible cost compatible with attaining set targets and obtaining predicted results, have made it possible to maintain the budget at a reasonably low level in spite of a considerable expansion of field activities into the Extension areas; high raises in staff emoluments; increases in the cost of equipment, supplies and services; and, not infrequently, an appreciable downtum in the value of the US dollar as against the other currencies in which OCP expenditures are defrayed.
See Annex 5 fora breakdown of staff by budget and unit (1992).
ACHIEVEMENTS AND IMPACT OF THE PROGRAMME
Examples of operational achievements
The Annual Transmission Potential (ATP) (1) dropped from 800 to below the acceptable level of 100 (2) in two thirds of the area under larviciding as early as 1978. Rapidly, a similar situation extended to the entire seven-country Original area, except the reinvaded zones in the west and in the south-east as well as in a few circumscribed zones where vector control had met with operational difficulties. Thus, in 1985 the last year of larviciding in the whole of the Original OCP area, more than 90% of the insect capture points reported ATPs less than 100 and in many cases zero.
Another important achievement in vector control has been the Program’ s successful handling of lowered susceptibility of the Simulium larvae to organophosphorus insecticides. Resistance is now overcome by rotation, according to a set application schedule, of temephos, phoxim and pyraclofos (all organophosphorus compounds),B.t. H-14 (a biological control agent), permethrin (a pyrethroid) and carbosulfan (a carbamate). Also, it is worth recording that the system of strict monitoring and surveillance of vector contro1, conducted by OCP during more than 15 years has shown no adverse impact oflarviciding: no disappearance of fish and invertebrate species has been recorded and the observed modifications have been of minor importance, and anyhow reversible.
As a result of larviciding, the prevalence of onchocerciasis is now insignificant in the major part of the Original Program area where the CMFL(3) has come close to zero. Furthermore, no onchocercal infections occurred in the Original Program area among children born since the start of vector control, except in the reinvaded zones and in the few areas where transmission temporarily relapsed. In those areas, only 1O to 20% of the infections expected in the absence of larviciding were recorded.
(1) The theoretical number of onchocercal larvae (L3) received by a person stationed at an insect capture point during one year.
(2) The upper tolerable limit for occupying the river valleys without risk of contracting serious onchocercal ocular lesions.
(3) Community Microfilarial Load: the geometric mean of microfilaria per skin snip among persons aged 20 years and more, including those with a zero count.
Impact on health
Thirty million people are now (1992) protected from onchocercal disease, i.e. 1O million in the Original Program area, where the threat has been virtually eliminated with the disappearance of the human parasite reservoir after 14 years of vector control, and 20 million in the Extension areas where transmission is halted by aerial larviciding and where the reservoir will disappear by the tum of the century. Nine million children born within the OCP area since Program operations began have been freed from the risk of contracting onchocercal blindness. And, by the year 2000, or even before, the number of children thus protected will have grown to 15 million. Also, of those seriously infected by onchocerciasis when the Program started, and therefore in grave danger of developing ocular manifestations, 1.25 million are no longer so, a figure expected to increase to 2 million around, or before, the year 2000. So far, in all more than 100,000 cases of blindness have been averted due to OCP control operations, a figure that will rise to 150,000 before the end of the century.
The use of large-scale ivermectin distribution as a means of morbidity control has been pioneered by the Program. Although, the drug did not live up to the early expectation that it could effectively interrupt transmission, ivermectin has proved itself to be a powerful agent with a pronounced clinical effect. The discomforts of onchocerciasis, such as itching, disappear rapidly and the risk of ocular manifestations, including blindness, is significantly reduced. The impact of ivermectin distribution, alone or in conjunction with aerial larviciding, is therefore highly beneficial to the communities under treatment, comprising more than half a million people within the OCP area.
Impact on socioeconomic development
According to the World Bank, the tillable “new lands” which have been, or are expected to be, made available as a result of onchocerciasis control followed by resettlement, are in the order of 150,000 km2 within the Original Program area, 50,000 km2 in the Southern Extension area and another 50,000 km2 in the Western Extension area, a total of 250,000 km2 (25 million hectares) for the entire Programme area. By 1991, already 150,000 km2 had been made ready for resettlement and cultivation, in part as a result of OCP operations. This should suffice to feed 10 million people. Further 100,000 km2 of fertile, riverain land in the Extension areas will become available before the end of the century, enough to feed another 7 million people if cultivated using traditional technological and agricultural practices.
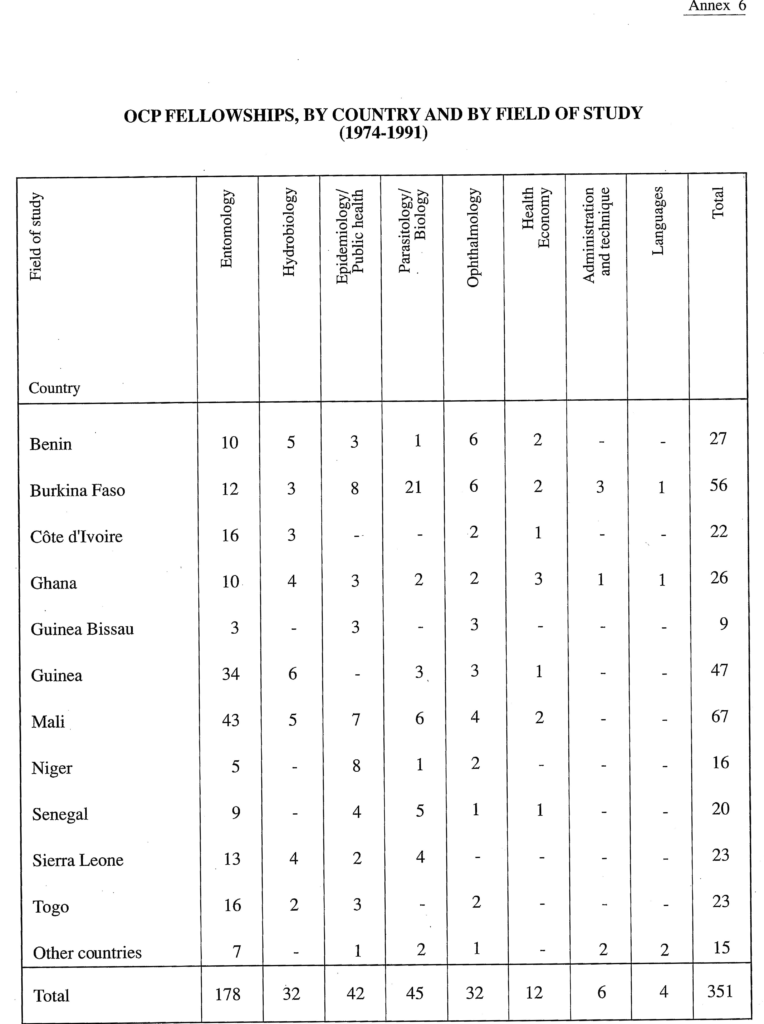
Impact of OCP training
OCP-conducted training operates on two fronts: by granting fellowships to nationals of the Participating Countries and by conducting in-service training and refresher courses for staff employed by the Program. As regards the former, please refer to Annex 6 which presents the distribution of OCP-awarded fellowships during the 1974-1991 period, by subject of study and by nationality of fellows. The gradual release of up to 800 OCP staff members, with good technical and managerial expertise, to national administrations and the return of several hundred candidates from OCP-funded fellowships, must, eventually contribute in no little measure to the strengthening of health and other services in the Participating Countries.
Impact in the field of research
Without the search for, and discovery of, replacement larvicides to overcome lowered susceptibility to temephos, Program-wide transmission control would have failed and OCP come to an ignominious end during the latter half of the eighties with the entire Program area eventually reverting to the situation prevailing before the start of aerial larviciding. The identification, vectorial role, and susceptibility to larvicides of the various forms and species of the blackfly as well as their geographical and seasonal distribution, have been subjects of intense investigation, all along the existence of the Program. The entomological map of the Simulium damnosum complex is now firmly drawn for the entire OCP area and the steady increase in the knowledge and understanding of the role in transmission, distribution and susceptibility to larvicides of the different vector species has allowed for rationalization of control activities and considerable economics in their implementation. Considerable progress has recently been made in developing a field-applicable DNA probe capable of distinguishing human from animal parasites.
Making ivermectin available for large-scale use in humans within a very short period, is another striking achievement of the Program. The impact of the OCP-conducted studies on the field applicability of the drug has been determining for its ever increasing use wherever human onchocerciasis prevails. The OCP/ TDR funded OCT/Macrofil project is intensifying its efforts to identify and test candidate compounds for their macrofilaricidal effect with good prospect of a drug becoming available within the foreseeable future. In this context, it is also worth mentioning that an immunodiagnostic test for detecting onchocerciasis in humans might soon be added to the investigative means of the Program.
Use of OCP expertise outside the Program area
The Onchocerciasis Control Program in West Africa is increasingly being viewed by those responsible for onchocerciasis control in other parts of the world, as a “resource facility” or “reference center” which can be called upon to provide expert advice. Staff members have thus been invited by authorities in non-OCP countries to assist in epidemiological/ophthalmological surveys and to ecommend on follow-up actions. Also, the OCP epidemiological model is under scrutiny for adaptation for use in the control of other public health problems.
END OF THE PROGRAMME
It is expected that the phasing-out period of the Program will start in 1998 and that OCP operations will cease by the end of this century.